
More Information
Submitted: 08 January 2020 | Approved: 11 January 2020 | Published: 13 January 2020
How to cite this article: Habib MH, Alkhodari KH. Coronary-intercostal steal syndrome, a rare connection between the left circumflex coronary artery and intercostal arteries: A case report. J Cardiol Cardiovasc Med. 2020; 5: 011-013.
DOI: 10.29328/journal.jccm.1001078
ORCiD: orcid.org/0000-0002-1537-9717
Copyright License: © 2020 Habib MH, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Intercostal artery; Left circumflex coronary artery; Angina; Steal syndrome

Coronary-intercostal steal syndrome, a rare connection between the left circumflex coronary artery and intercostal arteries: A case report
Mohammed H Habib1 and Khaled H Alkhodari2*
1Ph.D. Cardiology, Head of Cardiology and Cardiac Catheterization Department, Al-Shifa Hospital, Gaza, Palestine
2M.D, Al-Shifa Hospital, Gaza, Palestine
*Address for Correspondence: Khaled H Alkhodari, M.D, Al-Shifa Hospital, Gaza, Palestine, Tel: +00970599303107; Email: khaled.alkhodari@gmail.com
A 60-year-old female patient presented with typical anginal pain on exertion and relieved by rest for about one month. Percutaneous coronary angiography was done and showed an abnormal left circumflex coronary artery connecting to intercostal artery. Embolization of that abnormal connection was done successfully and the patient discharged from hospital after 24 hours. This case shows a new form of coronary steal syndrome. This cause could be missed if not put under the differential diagnosis of typical anginal pain with normal coronary arteries.
Congenital anomalies of the coronary arteries are present in about 1% of the general population [1]. The discovery of these anomalies is accidental during work up for angina pectoris. They can be looked up using invasive coronary angiography, or better using multidetector computed tomography coronary angiography [2]. There are many forms of coronary artery anomalies that are asymptomatic, non-significant to more complex dangerous forms that can lead to sudden cardiac death [1]. In this case we present a rare anomaly of the left circumflex coronary artery that resulted in myocardial ischemic symptoms on exertion and angiography showed that the left circumflex coronary artery is anastomosed with the intercostal arteries. In our knowledge, this case is the first time to be found in our country and it is not found in the literature.
A 60-year-old female patient complained from retrosternal chest heaviness that increases with exertion and relieved by rest, this pain radiated to left arm and its severity was 8/10. On examination, the patient looked anxious with good general condition, and stable vital signs. Chest examination and cardiovascular examination were normal. ECG was done it was normal, without ischemic changes. Complete blood count, kidney function tests, and lipid profile were normal.
A diagnostic invasive angiography for the coronary arteries was done and showed a bizarre anatomy of the left circumflex coronary artery as it not only supplies the heart but also it continues its way to supply the left side of chest wall. Otherwise, the coronary arteries are patent with no stenosis noticed, Figure 1.
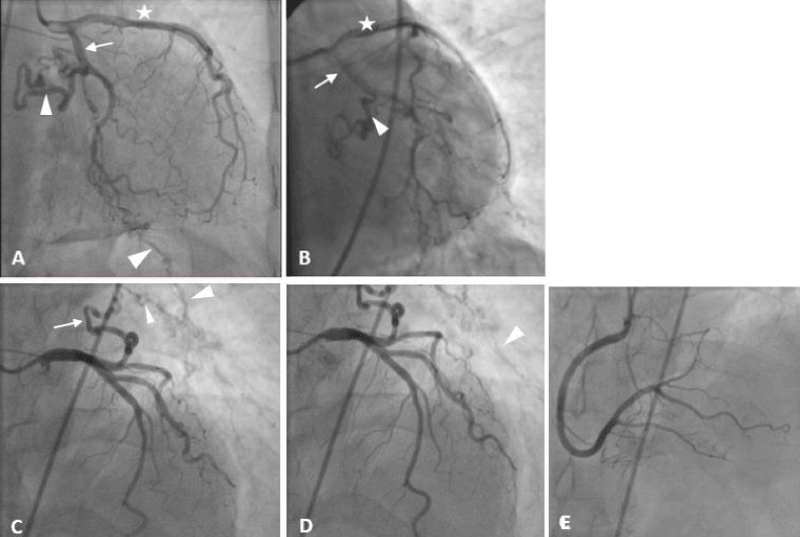
Figure 1: Percutaneous coronary angiography shows the anatomy of the coronary arteries. On A & B, the star refers to the left anterior descending artery, the arrow refers to the left circumflex coronary artery, and the arrow head refers to the abnormal branch of the LCX that continues to the intercostal arteries and the intercostal artery. C & D shows the course of the abnormal connection and the course of the intercostal artery. E shows the right coronary artery. Note that all coronary arteries have a patent lumen without stenosis./p>
Embolization of the left circumflex coronary artery after its heart-supplying branching was done using 3 coils, and control angiography showed total occlusion of the abnormal connection, Figure 2. Total procedure time was 45 minutes and the patient discharged from the hospital without complications 24 hours later.
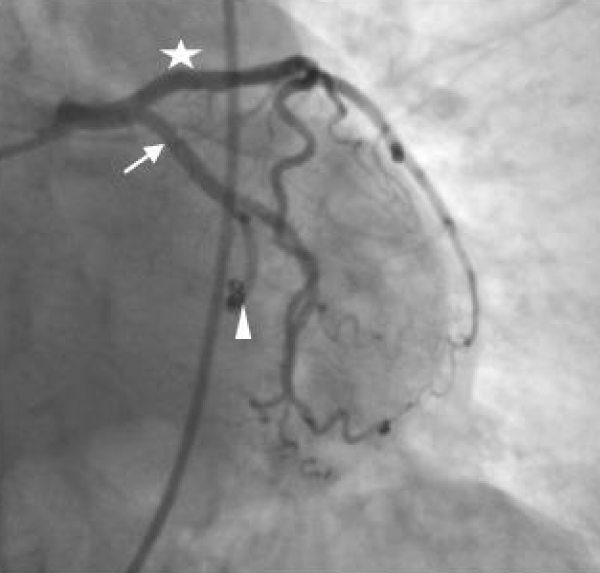
Figure 2: Percutaneous coronary angiography shows the anatomy of the coronary arteries. The star refers to the left anterior descending artery, the arrow refers to the left circumflex coronary artery, and the arrow head refers to the abnormal branch of the LCX that is now embolized using 3 coils.
Myocardial ischemia occurs when there is decrease in blood supply to heart muscle, there are many causes for the ischemia, ours is imbalance between oxygen supply and demand [3]. Congenital anomalies of the coronary arteries are rare, incidentally discovered during coronary angiography, or autopsies. The incidence of coronary artery anomalies increased from 0.3% in 1956 [4] to 2.33% in 2015 [5], in fact, the prevalence and the real incidence among general population is unknown and it could reach 5.6% [6]. This increase is mainly due to improve in diagnostic methods, from accidental finding in autopsies [4] to multi–detector row computed tomography coronary angiography [5] or percutaneous coronary angiography. Congenital anomalies of the coronary arteries are mainly asymptomatic and have no great impact on the person’s life, but sometimes it forms a life-threatening condition when there is anomalous origin of the left coronary artery from the pulmonary artery, large coronary arteriovenous fistulas, and those anomalies associated with a coronary artery coursing between the great vessels [6]. In young athletes, congenital coronary artery anomalies constitutes the second cause of sudden cardiac death, about 12% of deaths [1].
Although there are many forms of coronary artery anomalies reported in literature [1,4,6,7], the anomalies of the left circumflex coronary artery are rare, it constitutes about 0.3% of coronary artery anomalies [8]. In addition to that, no one has reported an anomaly like the case we present in which the left circumflex coronary artery continues to supply the left chest wall. This anomaly presents as myocardial ischemia like the idea of coronary steal syndrome, and coronary subclavian steal syndrome. On exertion, the blood flows through the left circumflex coronary artery to join the intercostal arteries in supplying the muscles of chest wall, resulting in relative myocardial ischemia [9]. Medical intervention mainly is indicated if the symptoms affects patient’s life, and it can be performed through the percutaneous coronary intervention and occlude the abnormal connection, using embolizing material like the coils [10].
According to variants of coronary artery, the management plan differs. Some variants mandates surgery to correct the anomaly like when the left coronary artery courses between the great vessels, and some are managed when they are symptomatic, but most of them require observation only [11].
Congenital anomalies of the coronary artery are rare but important to manage it they are symptomatic. They could present as arrhythmias, chest pain, or sadly sudden cardiac arrest. The management is different between the variants of the coronary artery some need open heart surgery, others require endovascular embolization as in this case, and many could be observed without intervention.
Consent
Verbal informed consent was obtained from the patient who was conscious and oriented to publish this case and all related materials.
- Angelini P, Velasco JA, Flamm S. Coronary anomalies: Incidence, pathophysiology, and clinical relevance. Circulation. 2002; 105: 2449-2454. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/12021235
- Koşar P, Ergun E, Öztürk C, Koşar U. Anatomic variations and anomalies of the coronary arteries: 64-slice CT angiographic appearance. Diagn Interv Radiol. 2009; 15: 275-283. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/19957241
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019; 72: 237–269.
- Alexander RW, Griffith GC. Anomalies of the Coronary Arteries and their Clinical Significance. Circulation. 1956; 14: 800-805. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/13374855
- Graidis C, Dimitriadis D, Karasavvidis V, Dimitriadis G, Argyropoulou E, et al. Prevalence and characteristics of coronary artery anomalies in an adult population undergoing multidetector-row computed tomography for the evaluation of coronary artery disease. BMC Cardiovasc Disord. 2015; 15: 1-10. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/26431696
- Silvia A, Baptista MJ, Araújo E. Cardiologia Congenital coronary artery anomalies. Port J Cardiol. 2018; 37: 341–350.
- Kastellanos S, Aznaouridis K, Vlachopoulos C, Tsiamis E, Oikonomou E, et al. Overview of coronary artery variants, aberrations and anomalies. World J Cardiol. 2018; 10: 127–140. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/30386490
- Wyeth RP, Arben S. Variant aortic sinusal origin of the left circumflex coronary artery. Int J Anat Var. 2014; 7: 109–111.
- Heusch G. Myocardial Ischemia: Lack of Coronary Blood Flow or Myocardial Oxygen Supply/Demand Imbalance? Circ Res. 2016; 119: 194–196. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27390331
- Mihatov N, Januzzi JLJ, Gaggin HK. Type 2 myocardial infarction due to supply-demand mismatch. Trends Cardiovasc Med. 2017; 27: 408–417. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/28438399
- Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, et al. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019; 73: e81–e192. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/30121239